How is Fully Ablative Laser Surgery used in the management pathway for acne scarring?
This is the stage of the acne scar management pathway illustrated below. It is highlighted in red.
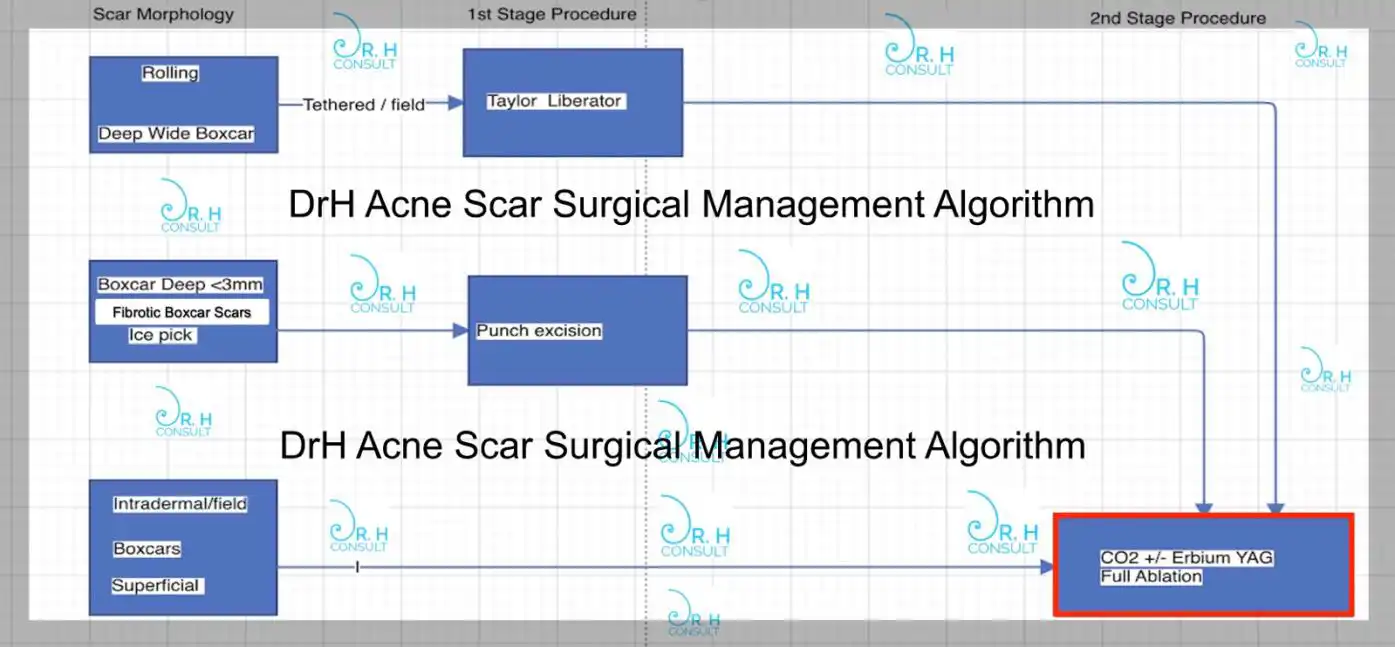
Dependent on the type of atrophic acne scar fully ablative laser resurfacing is a second stage or first stage procedure:
- For tethered rolling or boxcar scars it is a second stage procedure after Taylor Liberator Subcision.
- For fibrotic hypopigmented boxcar scars and ice pick scars it is a second stage procedure after punch excision of these scars.
- For intradermal boxcar or rolling scars (scars that are not tethered) it is the first stage and only stage that is required.
As always understanding which methodology relies always on appropriate classification of the scar type we are dealing with. This is why examination and appropriate diagnosis are essential first steps in managing acne scarring.
Everything procedure that Dr Hussein does to manage your acne scarring is based on this.
How do we treat this issue?
Dr Hussein is a specialist in laser skin surgery. He is the UK’s most experienced laser surgeon by case volume.
He uses the most advanced lasers to treat scarring.
Dr Hussein is the only UK laser surgeon with the skill, technology and experience to perform scar treartment in all skin types
Videos
Treatment at a Glance
Dependent on area treated. Please see the FAQs section.
Procedure Time
Typically three hours
Number of Treatments
Typically a single treatment
Downtime
Two weeks to three months




Frequently Asked Questions
A sedative will be administered and you will have a topical anaesthetic gel applied to the face for a period of around 45 minutes. Following this you will be taken in to the operating room for the main procedure.
The procedure will be performed using injected full face tumescent anaesthesia and will typically last for around one hour.
Following completion of your fully ablative resurfacing you will be taken to the recovery room. After around 30 minutes of monitoring you will be checked by Dr Hussein and the Nurse in charge. After satisfactory checks you will be allowed to leave and travel home.
To fully recover takes approximately 3 months (Wedding ready as DrH likes to call it!)
Full recovery means:
- Redness settling to baseline
- Hyperpigmentation settling to baseline
- Textural roughness from inflammation (grainy/sandpaper/orange peel texture) settling completely
In some cases it is possible to experience elevated skin sensitivity for up to 6 months. Darker skinned patients may require longer than three onths and even up to six months for full pigmentation recovery.
- Weeping and dripping in the first 5 days of recovery.
- Swelling of the face that will last for up to 4 days.
- 3 months of decreasing redness. Itch can occur from day 3-4 onwards.
- It is normal to experience stinging while washing the face for the first 5 days. This decreases day by day.
- Post inflammatory hyperpigmentation. This is temporary and can be expected to occur in fully ablative resurfacing. It resolves over 3 months spontaneously in the majority of cases
Complications of this procedure are decribed at length in the consent and pre-reading literature but can be summarised as follows:
- Infection
- Scar
- PIH
- Hypopigmentation
- Erosive Pustular Dermatosis
- Prolonged Redness
- Dealayed Healing
- For the first 14 days following your fully ablative resurfacing procedure DrH will monitor you daily using the Virtual Ward Round. This involves the use of daily photo checks and direct communication with the patient.
- Following this a twice weekly photo monitoring for the following 2 weeks till day 28 allows Dr Hussein to monitor progress.
- At three months in clinic review is scheduled. Typically after this review you can be discharged.
- Topical anaesthesia is not painful
- Tumescent anaesthesia is painful due to multiple small needle pricks
- Following the tumescent the procedure is largely pain free but heat and sting can be felt at the edges of the face
- Sunburn sensation is normal for around 24 hours post procedure
- Washing the face twice daily is required and this will sting. The first day wash stings most. This then progressively wears off so that by day 5 washing is not uncomfortable at all.
- Eye shield insertion is not painful. However anaesthetic eye drops sting for 5 seconds after application. This is typically like a getting soap in the eye sensation that lasts for 5 seconds before settling completely
- Click on the booking form link
- Fully complete the booking form
- By giving us complete information you will help us appropriately assess your concerns
- Information is not used for any marketing purpose – It is essential medical information
- My team is small and busy and do not take random phone calls.
- Follow the booking form process and you will be duly contacted by Harriet. She will arrange your consultation.
- Following consultation your treatment can be booked. This is usually no earlier than 2 weeks following the consultation. This time is important to allow full consideration of the procedure by the patient. This is a part of the GMC guidelines and we strictly adhere to it. Exceptions can be made whereby international travel or mitigating circumstances require. However it is not something Dr Hussein encourages.
- Consultation is compulsory prior to treatment preferably in person but can be arranged online – Cost £200
- Fully ablative resurfacing for acne scarring costs £4250
- The medical pack containing facewash, ointments and prophylactic medication for your procedure cost £90
- End to end cost of acne scar treatment requiring fully ablative laser resurfacing only will cost £4540
In mixed pattern scarring:
- If punch excision is required prior It will be the standard £2250 charge on the website.
- If Taylor Liberator is required prior to resurfacing it will be the standard £2250 charge on the website.
- If both Taylor Liberator and multiple punch excisions are required before resurfacing they can be combined into one procedure performed in a single session. Combined Taylor Liberator and Punch Excision costs £2750.
Combination of procedures will be determined by examination during the consultation. If the consultation is online Dr Hussein requests well lit high resolution photos to be sent prior to consultation. From experience Dr Hussein can make a good judgement of what is required from photos. Absolute confirmation will be made on physical examination.
If punch excision is required there must be a window of maximum 4-6 weeks before full ablation is undertaken. This is because optimum results for the punch excision revision scars require full ablation to be performed within this time frame. This must be taken into account during the procedure planning process.
It is Dr Hussein’s usual practice to allow at least a 2-3 week gap between Taylor Liberator and resurfacing. Given that Taylor Liberator subcision and fully ablative laser are mutually independent procedures for different aspects of scarring there is no fixed timeframe between them.
Why do we perform fully ablative laser resurfacing for acne scarring?
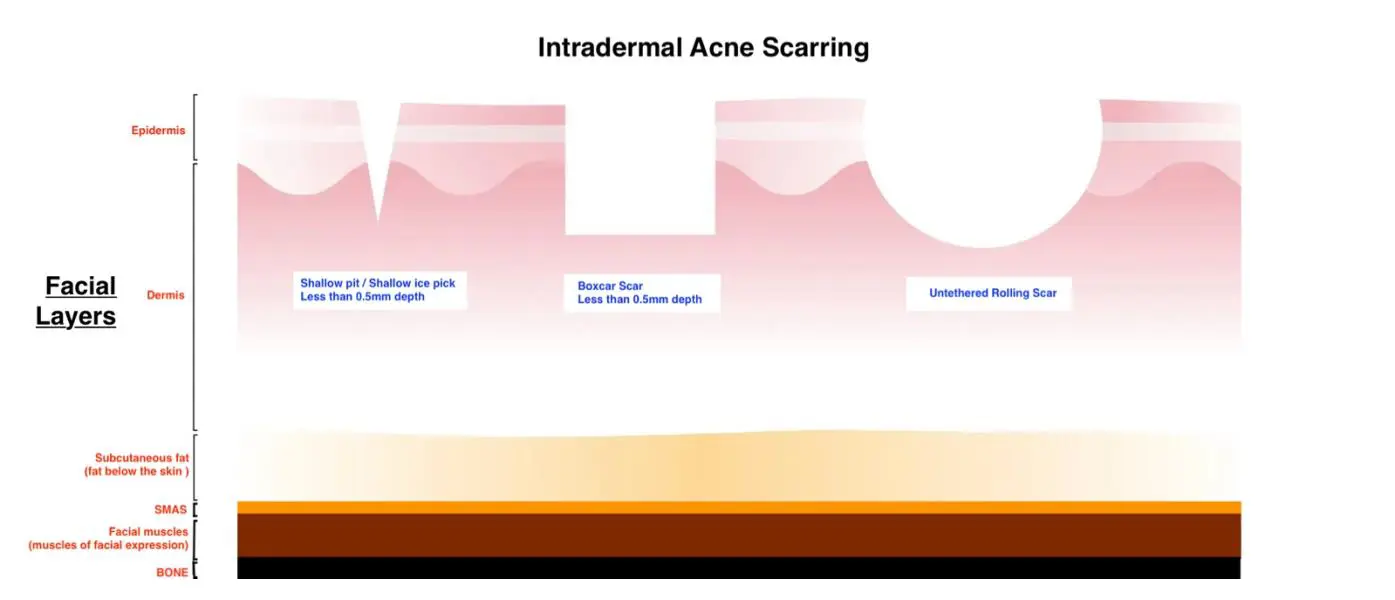
Full ablation is performed to remodel the outer surface of the skin that is affected by intradermal scars. Intradermal scar means – a scar within the skin. Look at the diagram below for a visual aid to see what we mean by scars within the skin.
This means scars which are effectively wholly contained within the skin layer. These scars have no component that stretches below the skin. Fibrous tethering anchors the skin to the SMAS layer and therefore by definition is not an intradermal scar. Deep ice pick scars or boxcar scars must be cut out (punch excision) to create a new shallow scar less than 0.5mm in depth within the skin that can be then tackled by full ablation laser resurfacing. Hence full ablation is the second stage for management of tethered scars and deep icepick/fibrotic deep boxcar scars.
Full ablation laser resurfacing essentially allows us to remodel the full skin surface. Unlike fractional ablative resurfacing where only holes are drilled in a small portion of the skin. When it comes to effective modalities for intradermal atrophic acne scar treatment full ablation is the gold standard.
Acne scarring is a large field defect of the skin and as such to be treated most effectively requires a full ablation to remove and remodel the entire skin surface and depth to give the greatest remodelling of the skin. With full ablation performed on the correct scar type (intradermal scars less than 0.5mm in depth) a consistent improvement of on average 70% can be reliably achieved, case after case.
There is no other method available today that can reliably deliver the degree of improvement on intradermal atrophic acne scarring. Full ablation is and always has been the most effective way of treating these scars.
Why is this issue hard to treat effectively often?
Partial remodelling of the skin with fractional laser is the common method used all over the world in management of intradermal acne scars. It is not however the gold standard. Fractional laser and other methodologies for treatment of acne scars are common for the following reasons:
The reason why we perform this is because in order to perform fully ablative resurfacing in a safe and effective way requires a great deal of skill and training in the use of laser. Dr Hussein is one of five dermatological surgeons worldwide who have extensive experience (50 plus acne scar cases a year treated by full ablation is what is deemed to be experienced enough to teach in the UK).
Dr Hussein performs well over 100 full ablation acne scar full ablation laser surgeries a year. This makes Dr Hussein the only real choice for full ablation laser in the United Kingdom.
As one of the most experienced skin laser surgeons worldwide Dr Hussein can perform full ablation with CO2 laser (Lumenis Ultrapulse Alpha), Erbium YAG laser (Sciton Joule X double Erbium YAG – built bespoke for Dr Hussein and the only device of its kind in the UK) and a combination of both.
Full ablation laser resurfacing of the skin also requires the appropriate equipment. Very few lasers can be used effectively for deep full ablative skin resurfacing. The ability of an ablative CO2 or Erbium YAG laser to be used for deep full ablation depends on its power output, scanner design and ability to modulate pulse width effectively. It also requires the knowledge of the performing skin surgeon on how to manipulate these factors effectively and safely to achieve the optimum outcome.
Worldwide it is known by all dermatologists and plastic surgeons that the two gold standard lasers for fully ablative skin resurfacing are:
- Lumenis Ultrapulse Alpha CO2 (laser released in 2023)
Dr Hussein is the first Dermatologist in Europe to acquire the new Lumenis Ultrapulse Alpha - Sciton Joule X Erbium YAG (laser released in 2020)
Dr Hussein owns and operates both devices and is a worldwide authority in fully ablative laser surgery.
How do derma / aesthetic clinics usually treat this condition?
Microneedling, radiofrequency microneedling, chemical peels, fractional non ablative laser and fractional ablative laser are all common methods used all over the world in management of intradermal acne scars.These are not the gold standard. These methodologies are used for the following reasons.
- Cheaper to provide.
- Low improvement in the scarring is the trade-off for low risk procedure
- Most dermatologists and plastic surgeons worldwide have not been trained and do not have the caseload to sustain a practice that uses full ablation as a mainstay technique in acne scar management.
- Acne scarring is not taken seriously by most clinics.
- Low risk procedures are repeated again and again with low success. However this is profitable.
- Training in microneedling, radiofrequency microneedling, and peels takes days. One does not have to be even medically trained to perform this. Understanding and being able to use surgical ablative lasers effectively required years of experience and training in medicine and skin laser surgery.
Why is this not effective for the patient?
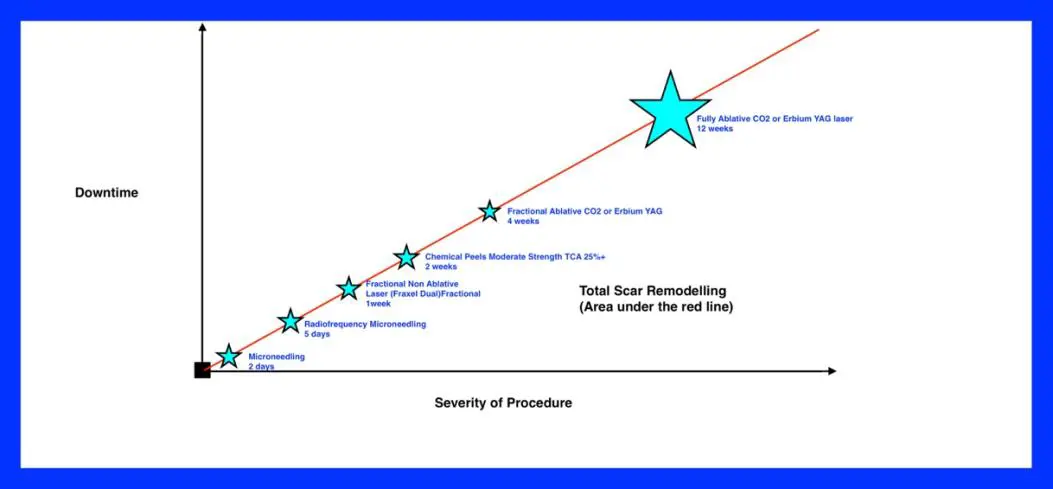
If one looks at the chart below we will understand why fully ablative resurfacing is the gold standard in acne scar management.
In order to trigger reconstruction and remodelling within the skin. The skin cells that manufacture collagen (Dermal Fibroblasts) must be activated to do so. Atrophic scars are indented scars caused by inflammation that has destroyed the skin collagen scaffold. This then results in the indented scars that form the majority of acne scars. In order to improve the scar height new collagen must be produced by the dermal fibroblasts.
In order to stimulate collagen production and inflammation must be triggered withing the skin. From an acne scar treatment perspective this means that we must give a controlled injury to the skin.
In acne scar treatment methods of controlled injury include:
- Microneedling (trauma to the skin caused by micro lacerations to the skin)
- Radiofrequency Microneedling (trauma from micro lacerations and thermal injury combined)
- Chemical Peels (Chemical burn to the skin)
- Laser (Light induced thermal burn of the skin)
The duration and severity of the inflammatory process dictate the level of improvement in scarring as this essentially as these are the two factors that combine together to give the duration and extent of collagen remodelling. The lower down the chart we are in terms of downtime and severity the less we can expect the dermal fibroblast collagen remodelling of the skin to endure. This means lower improvement in acne scarring.
Greater Improvement in acne scars = Greater Inflammation and Greater Duration = Greater Extent of Injury
How do WE treat this issue?
Dr Hussein uses fully ablative laser resurfacing. The diagram below helps give a visual explanation of how ablative and non ablative lasers treat the skin. Fully ablative laser resurfacing is highlighted in the red box.

When Dr Hussein uses deep fully ablative resurfacing he uses CO2 laser or Erbium YAG laser. For very deep scarring he has pioneered a very deep form of laser resurfacing called COMBINED FULLY ABLATIVE LASER RESURFACING. This method uses both the Lumenis Ultrapulse Alpha CO2 laser and the Sciton Joule X Erbium YAG lasers in the same procedure. He has also pioneered in the use of this technique all patients including darker skin types. Use of combined resurfacing technique in a darker skin type can be seen in the video below.
Deep fully Ablative Resurfacing has the following distinct advantages when compared to fractional ablative resurfacing.
- The whole surface area of the skin affected by intradermal acne scars can be treated. The ablation will remove the epidermal layer in its entirety and then remodel the dermal layer in which the scars are contained. The whole scar containing deeper dermal tissue can be fully remodelled effectively. Fractional laser at best when used in its microfractional array mode (this is the mode required to treat the deeper dermis affected by the scars) will only allow for a maximum of 20% of the skin surface area to be treated. This means partial treatment of scars and missing some scars altogether. This is why the improvement in the scarring is much greater in fully ablative resurfacing. Essentially because it allows for whole surface epidermal and deep dermal scar remodelling.
- The prolonged downtime and severity of full ablation allow for extensive collagen remodelling over a longer duration This can be seen in the study from below. The graph is taken from a study by Orringer et al published in the journal of Dermatalogic Surgery.
Triggering type 1 and 3 production is the greatest predictor of clinical effectiveness in any type of laser resurfacing.
- Fully Ablative laser resurfacing triggers double the level of peak collagen induction when compared with fractional ablative laser. Not only is the extent of collagen production much greater (in fully ablative laser surgery vs fractional ablative laser surgery), it is also greater for a much more sustained period of time. This is the foundation for the downtime vs severity chart for different methofs of acne scar management that you see in this section. Fully ablative laser has been the gold standard since it was developed in the late 90’s. Dr Hussein has himself used both techniques and has performed both techniques over the last decade. The biggest improvements in intradermal scarring have always been from full ablation. The problem is that since the advent of fractional lasers post 2005 and the rapid shift towards them the skills and experience to perform full ablation have been all but made extinct in dermatologists and plastic surgeons.
- One treatment is all that is required. Deep fully ablative resurfacing is the only technique that can provide a 70% height and surface improvement in atrophic non – fibrosed intradermal acne scars of <0.5mm depth. The natural disadvantages that come with this are:
- Prolonged downtime when compared to fractional ablative laser
- Prolonged redness and social inconvenience caused by recovery appearance
- Need for at least 12-14 days off work post procedure
- Greater risks in infection post procedure but this is mitigated by appropriate medication prophylaxis and woundcare
In summary here typical level of benefit that can be expected from deep fully ablative laser resurfacing is 70%. The typical benefit from aggressive fractional laser resurfacing is 20%. Just adding fractional treatments together will not summate to full ablation. Remember there is a law of diminishing returns. Two fractional laser resurfacings do not equal 40% benefit. 20% from the first fractional. Then 20% on the residual scarring after the first fractional resurfacing.
- In short Dr Hussein uses deep fully ablative resurfacing in over 100 cases of acne scarring per year. This makes him the only UK laser surgeon with sufficient caseload, skill and experience to use this method safely and effectively. There is no other dermatologist or plastic surgeon in the UK with Dr Hussein’s level of experience in full ablation.
How can we evidence our approach is better?
It is a medically accepted fact in all literature regarding acne scar management techniques that deep ablation is the procedure that will give the greatest improvement in intradermal atrophic acne scarring.
Superiority of Fully Ablative Laser Resurfacing vs Fractional resurfacing and Non Ablative Resurfacing
Please look at the yellow highlighted section from the abstract of this key article on laser resurfacing. The full article can be accessed from the American Academy of Dermatology by clicking on this link.
Fully ablative Laser Resurfacing has long been established as a superior method of skin resurfacing in producing superior results. All dermatologists and plastic surgeons know this. However fractional resurfacing and non-ablative resurfacing are safe and lower risk methods. They do not yield comparable results. DrH is an expert in fully ablative laser surgery.
DrH is the most experienced fully ablative laser surgeon in the UK by case volume. He is experienced in all modalities of full ablation and can treat all skin types.
How can we evidence our approach is better?
It is a medically accepted fact in all literature regarding acne scar management techniques that deep ablation is the procedure that will give the greatest improvement in intradermal atrophic acne scarring.
Superiority of Fully Ablative Laser Resurfacing vs Fractional resurfacing and Non Ablative Resurfacing
Please look at the yellow highlighted section from the abstract of this key article on laser resurfacing. The full article can be accessed from the American Academy of Dermatology by clicking on this link.
Fully ablative Laser Resurfacing has long been established as a superior method of skin resurfacing in producing superior results. All dermatologists and plastic surgeons know this. However fractional resurfacing and non-ablative resurfacing are safe and lower risk methods. They do not yield comparable results. DrH is an expert in fully ablative laser surgery.
DrH is the most experienced fully ablative laser surgeon in the UK by case volume. He is experienced in all modalities of full ablation and can treat all skin types.

Through experience and the use of state-of-the-art equipment (Lumenis Ultrapulse Alpha CO2 & Sciton Joule X Erbium YAG) he is able to perform the most aggressive resurfacing for acne scarring.
Through extensive experience, routine monitoring and appropriate peri-procedural prophylaxis his complication rate is extremely low.
If you are going to have full ablation in the UK then DrH is the UK leader.